Half of all heart attacks in the United States occur in people with perfectly normal cholesterol levels. How can that be?
Currently, your annual lipid panel reports four numbers. Total cholesterol. LDL. HDL. Triglycerides.
For decades this has been the standard. But this four-number snapshot was designed in an era before scientists understood the full picture of heart disease. We now know that two of the most powerful predictors of a heart attack: Lipoprotein(a), or Lp(a) & Apolipoprotein B, or ApoB, are not on it.
This article explains what Lp(a) & ApoB are, how they work at a biological level, who is most at risk & why even aggressive cholesterol treatment may not be enough if these markers go undetected & unmanaged.
While it is a denser article, readers will find concepts approachable for all levels: we wrote this with all audiences in mind.
The Architecture of a Heart Attack
To understand why standard cholesterol tests can miss so much, we must first understand what actually causes a heart attack. Heart attacks are caused by blood flow blockage from the build-up of waste & fats inside arteries, specifically arterial walls. This phenomenon is called “atherosclerosis”.
Particles carrying cholesterol & fat inside the bloodstream, known as lipoprotein particles, can become atherogenic (promoting atherosclerosis aka heart attacks), such as low-density lipoprotein (LDL), a mainstay of cholesterol testing. They penetrate & become trapped within the endothelium, the thin lining of your coronary arteries.
Once trapped, they oxidize. The immune system responds with inflammation to combat the intrusion; macrophages (specialized white blood cells) rush in, consume the particles & transform into foam cells upon cell death. These are known as the cellular building blocks of plaque.
Over years, this process builds. Plaque grows, hardens, or remains soft & lipid-rich. When a vulnerable plaque ruptures, a clot forms. Blood flow is cut off. That is a heart attack.
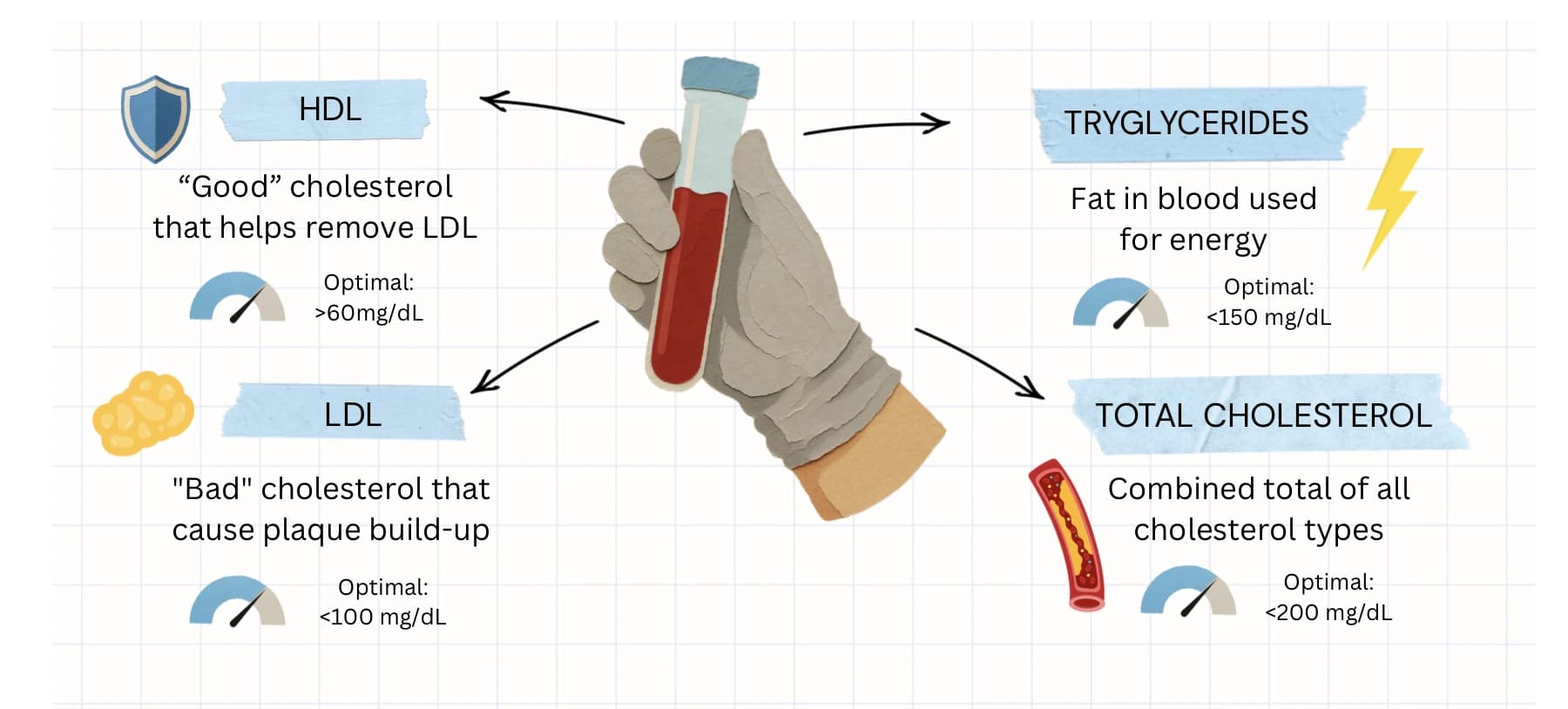
A standard lipid panel reports just four numbers: HDL, LDL, triglycerides & total cholesterol.
The standard LDL cholesterol test measures the amount of cholesterol floating inside these particles. What it does not measure is how many particles there are, or whether you are carrying a particularly dangerous variant that accelerates every step of this process.
Said another way, standard lipid panels measure the total volume of cholesterol. However, the exact count & size of these particles are better indicators of your true cardiovascular risk.
One can have normal cholesterol levels but still have a dangerous abundance of small, dense particles, or more inflammatory particles, that accelerates the process of atherosclerosis.
First, What Is Lp(a) & Why Is It Different?
Lipoprotein(a) is an LDL-like particle with an additional protein called apolipoprotein(a).
The extra protein mimics the body’s natural clot-dissolving enzyme & can competitively inhibit your body’s ability to break down dangerous clots. Making Lp(a) doubly dangerous: it is simultaneously atherogenic (builds plaque) & thrombogenic (promotes clotting).
New research from Mount Sinai published in the European Heart Journal—Cardiovascular Imaging (2026) found that patients with high Lp(a) develop a distinct type of plaque: less calcified, more lipid-rich & significantly more prone to rupture than the plaque seen with elevated LDL cholesterol.
High-Lp(a) plaques also trigger the release of tissue factor, an activated clotting protein that makes any resulting clot more resilient & harder for the body to dissolve.
The biological cascade, as one Mount Sinai researcher describes it: “The plaque becomes more likely to rupture, more likely to get inflamed, and then the inflammatory cells release tissue factor. That leads to a big clot that is more resilient and doesn’t dissolve easily.”
Lp(a) Is Genetic, You Cannot Lifestyle Your Way Out of It
As much as 90% of the variation in Lp(a) levels between individuals is genetically determined, meaning it is controlled almost entirely by your genes. The inheritance pattern is autosomal co-dominant: if one parent carries the elevated variant, each child has a 50% chance of inheriting it.
Statins cannot lower Lp(a). No dietary change meaningfully reduces it. No amount of exercise resets it. You can almost think of it as a genetic fingerprint: present from birth & largely invisible unless specifically tested.
Approximately 1 in 5 Americans carries elevated Lp(a) levels above 50 mg/dL, making it the most common genetic cholesterol abnormality linked to early cardiovascular disease. Unfortunately, fewer than 5% of Americans have ever been screened for it, because Lp(a) is not included in a standard lipid panel.
Who Is Most at Risk: The Racial Disparity in Lp(a)
Black Americans face the highest prevalence of elevated Lp(a) of any racial or ethnic group. In a large JACC study of over 13,000 patients who underwent Lp(a) testing, 62.6% of non-Hispanic Black patients had Lp(a) levels above 50 mg/dL, compared to 30.7% of Mexican patients. After statistical adjustment, Black individuals had 2.46 times the odds of elevated Lp(a) compared to white patients.
South Asian Americans are another high-risk population. Despite reporting healthier diets, lower alcohol use & comparable physical activity levels to other groups, South Asians develop atherosclerosis up to a decade earlier than the general U.S. population. A 2026 Northwestern Medicine study following 2,700 adults found that South Asian men at age 45 already showed rates of high cholesterol & triglycerides dramatically exceeding other groups, with researchers explicitly recommending Lp(a) screening before midlife.
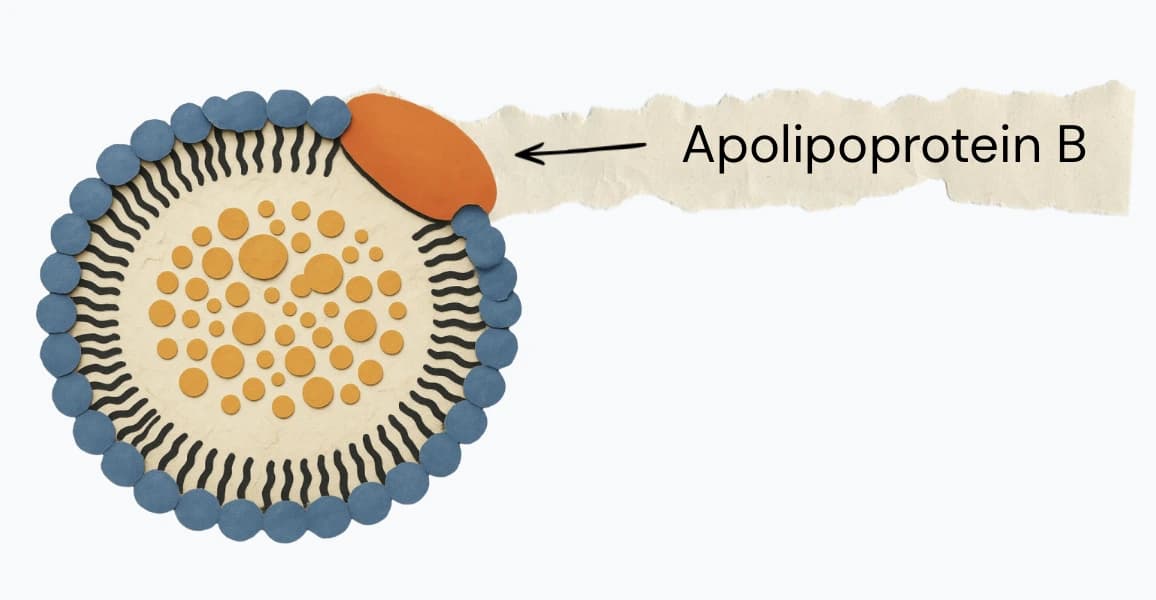
Every atherogenic lipoprotein particle carries exactly one ApoB molecule.
Next, What Is ApoB?
Apolipoprotein B is a structural protein. There is exactly one ApoB molecule on every single atherogenic lipoprotein particle in circulation. That is every LDL, every VLDL, every IDL, every Lp(a).
This means that measuring ApoB gives you something LDL cholesterol cannot: a direct particle count of how many artery-damaging particles are circulating in your blood.
The distinction matters because two people can have the same LDL-C number but wildly different particle counts. A person with many small, dense LDL particles may carry far more atherogenic particles than someone with fewer, larger ones, all at the same measured LDL cholesterol level. Their risk profile would differ significantly. But their standard lipid panel would look identical.
A 2007 prospective study in Arteriosclerosis, Thrombosis, and Vascular Biology followed 9,231 individuals for 8 years. Women in the highest ApoB tertile had hazard ratios of 2.6 for myocardial infarction. Men showed hazard ratios of 2.4, consistently outperforming LDL-C as a predictor across both sexes & multiple cardiovascular endpoints (p < 0.001).
Despite this, ApoB is still not part of the standard cholesterol panel. A 2024 Circulation review noted that ApoB measurement has failed to become routine largely due to inconsistent clinical guidance & the absence of established treatment targets.
How It Should Reshape Your Thinking of Heart Health Scores
Here is where clinical nuance comes in: knowing that blood marker concentrations can vary vastly in what it predicts & that your LDL target is not a universal number. It depends entirely on your risk profile.
For a healthy adult with no history of cardiovascular disease & no risk-enhancing factors, an LDL below 100 mg/dL is generally considered acceptable. But for a high-risk patient: someone with established plaque, prior cardiovascular events, diabetes, or high Lp(a), the threshold drops dramatically.
According to the 2019 ESC/EAS Guidelines & subsequent clinical trial evidence, the LDL target for very high-risk patients is below 55 mg/dL (1.4 mmol/L). To stabilize lipid-rich, vulnerable plaques & promote regression, cardiologists now target LDL-C levels between 50 & 55 mg/dL.
For patients who cannot reach these targets on statin therapy alone, Repatha (evolocumab) is a PCSK9 inhibitor that blocks the liver protein responsible for degrading LDL receptors, allowing more receptors to recycle & clear LDL from the bloodstream. It has been shown in the 2025 VESALIUS-CV trial to reduce major adverse cardiovascular events by 25% & heart attack risk by 36%, achieving a median LDL of 45 mg/dL in high-risk patients.
This means that if you are a patient on statin with an LDL of 80 mg/dL who has existing plaque, you may still be well above your therapeutic goal.
The Question to Ask at Your Next Physical
Here are the three things to request the next time you see your doctor:
- An Lp(a) test. This is a single one-time blood test that should be done in every adult’s lifetime according to European Atherosclerosis Society consensus guidelines. If elevated, it should inform family screening of first-degree relatives.
- An ApoB test. This is inexpensive, widely available but not yet standard of care despite compelling evidence that it outperforms LDL-C as a predictor of cardiovascular events.
- A risk-stratified LDL conversation. Specifically, what LDL target is appropriate for your risk profile.
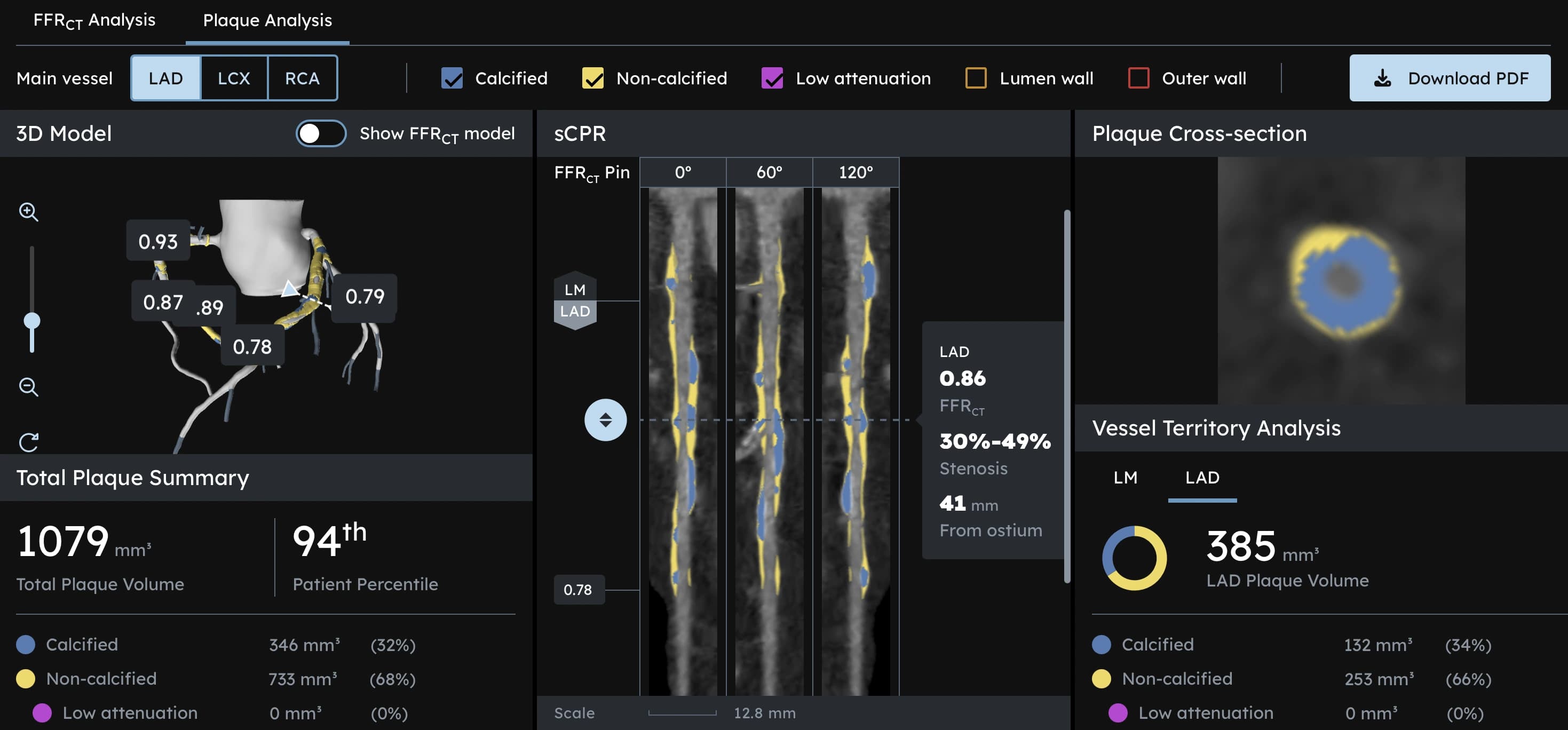
If you want to go beyond blood markers & actually see what is building inside your coronary arteries, a CCTA HeartScan provides a non-invasive insight of coronary plaque, detecting both calcified & soft, non-calcified plaque that no blood test can reveal. For patients with elevated Lp(a) or high ApoB, it is the next logical step: not guessing at risk, but measuring it directly.
Further Reading
1. The most comprehensive peer-reviewed synthesis of Lp(a) biology, genetics, pathophysiology, and emerging clinical evidence available. “Lipoprotein(a): A Genetically Determined, Causal, and Prevalent Risk Factor for Atherosclerotic Cardiovascular Disease: A Scientific Statement From the American Heart Association.” AHA Journals
2. Physiological explanation for why particle count outperforms cholesterol mass as a predictor (essential foundational reading for understanding the limits of LDL-C). “Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk.” Journal of the American Heart Association
3. Evidence on Repatha’s cardiovascular outcomes benefit in primary prevention, establishing the 45 mg/dL LDL achieved target in a high-risk population. “Evolocumab in Patients without a Previous Myocardial Infarction or Stroke.” NEJM
References
[1] Gidding, S. S., Wiegman, A., Groselj, U., Freiberger, T., Peretti, N., Dharmayat, K. I., Daccord, M., Bedlington, N., Sikonja, J., Ray, K. K., Santos, R. D., Halle, M., Tokgözöglu, L., Gutiérrez-Ibarluzea, I., Pinto, F. J., & Geanta, M. (2022). Paediatric familial hypercholesterolaemia screening in Europe: public policy background and recommendations. European Journal of Preventive Cardiology, 29(18), 2301–2311. link
[2] Fang, S., Deng, C., & Zhao, R. (2025). Lipoprotein(a) and High-Risk Coronary Plaques: Mechanisms, Characteristics, and Emerging Therapeutic Strategies. Reviews in Cardiovascular Medicine, 26(10), 44003. link
[3] Bohula, E. A., Marston, N. A., Bhatia, A. K., De Ferrari, G. M., Leiter, L. A., Nicolau, J. C., Park, J. G., Kuder, J. F., Murphy, S. A., … VESALIUS-CV Investigators. (2026). Evolocumab in Patients without a Previous Myocardial Infarction or Stroke. The New England Journal of Medicine, 394(2), 117–127. link
[4] Glavinovic, T., Thanassoulis, G., de Graaf, J., Couture, P., Hegele, R. A., & Sniderman, A. D. (2022). Physiological Bases for the Superiority of Apolipoprotein B Over Low-Density Lipoprotein Cholesterol and Non-High-Density Lipoprotein Cholesterol as a Marker of Cardiovascular Risk. Journal of the American Heart Association, 11(20), e025858. link
[5] Tsimikas, S., Fazio, S., Ferdinand, K. C., Ginsberg, H. N., Koschinsky, M. L., Marcovina, S. M., Moriarty, P. M., Rader, D. J., Remaley, A. T., Reyes-Soffer, G., Santos, R. D., Thanassoulis, G., Witztum, J. L., Danthi, S., Olive, M., & Liu, L. (2018). NHLBI Working Group Recommendations to Reduce Lipoprotein(a)-Mediated Risk of Cardiovascular Disease and Aortic Stenosis. Journal of the American College of Cardiology, 71(2), 177–192. link
[6] Thanassoulis, G. (2019). Screening for High Lipoprotein(a). Circulation, 139(12), 1493–1496. link
[7] Borén, J., Chapman, M. J., Krauss, R. M., Packard, C. J., Bentzon, J. F., Binder, C. J., Daemen, M. J., Demer, L. L., Hegele, R. A., Nicholls, S. J., Nordestgaard, B. G., Watts, G. F., Bruckert, E., Fazio, S., Ference, B. A., Graham, I., Horton, J. D., Landmesser, U., Laufs, U., Masana, L., … Ginsberg, H. N. (2020). Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. European Heart Journal, 41(24), 2313–2330. link