Across large population studies, gastrointestinal symptoms are common even in people who have never been told they have a “digestive disease.” Because many never hear a diagnosis, few move beyond over-the-counter remedies, elimination diets, and guesswork, despite how much the symptoms shape their day-to-day decisions.
The Quiet Epidemic of Everyday Digestive Issues
If you regularly feel bloated after meals, need to plan your day around the nearest bathroom, or live with heartburn, you're not alone.
Large international studies suggest that more than 40% of people worldwide have ongoing functional gut disorders such as irritable bowel syndrome (IBS) or functional dyspepsia, which can cause pain, bloating, constipation, and diarrhea without an obvious structural disease on basic tests.
In the United States, digestive problems drive over 100 million outpatient visits every year, even though many people still never get a clear diagnosis and simply “live with it.”
For many adults, this often becomes background noise in daily life; a constant negotiation with food, social plans, and travel.
Mapping Digestive Issues to the GI
Digestive problems cover a wide spectrum, but are frequently divided into the following:
| Issue Type | Symptoms and Impact |
|---|---|
| Upper GI symptoms | Burning behind the breastbone, stomach pain after eating, early fullness, or nausea, often grouped under dyspepsia or GERD (acid reflux). These symptoms may change what, when, and how much people eat and can interfere with sleep and exercise. |
| Lower GI symptoms | Cramping, bloating, diarrhea, constipation, or an unpredictable mix of both, as seen in IBS and other gut–brain interaction disorders. People often avoid social events, travel, and certain jobs because they need constant bathroom access. |
| Alarm Features | Unintentional weight loss, blood in the stool, severe persistent pain, fevers. These can signal inflammatory bowel disease, cancers, or serious infections and typically warrant urgent investigation. |
Have Digestive Problems Really Increased, and Why?
While past data is sparse, what we do know is that functional gastrointestinal disorders (like IBS and functional dyspepsia) affect a very large and clinically significant portion of the population today.
In a multinational survey using standardized Rome IV criteria, more than 40% of respondents met criteria for at least one functional gut disorder, with substantial impact on well-being and work.
But short of humans being maladapted for eating, we can attribute this population-wide struggle to a few lifestyle and psychosocial factors:
- Diet and fatty foods. Studies in various populations have linked high-fat diets to more dyspepsia and IBS symptoms.
- Low physical activity. Lower activity levels correlate with higher rates of IBS and dyspepsia in some cohorts.
- Smoking and other habits. Cigarette use has been associated with more IBS in certain studies.
- Stress and anxiety. Functional gut disorders are tightly linked with anxiety and other psychological factors, which influence symptom severity and health-care seeking.
At the same time, organic diseases such as Crohn's disease, ulcerative colitis, and certain digestive cancers remain important causes of symptoms in middle adulthood, and some data suggest that inflammatory bowel disease has become more common in many regions over recent decades.
This mix of high rates of “functional” symptoms plus a meaningful risk of structural disease creates exactly the uncertainty many people feel: “Is this just my sensitive gut, or is something actually wrong?”
Why Many People Avoid Testing (Even When They're Curious)
If you've ever thought, “I'd like to know what's going on in there, but I don't want a tube down my throat or a bunch of radiation,” you're not alone. The most common barriers to avoiding or postponing treatment include:
- Fear of invasive tests like colonoscopy or endoscopy
- Worries about radiation exposure from repeated CT scans
- Confusion about what different scans actually show
- Past experiences of being told “everything is normal” despite ongoing symptoms
This is where modern magnetic resonance imaging (MRI) has quietly changed the landscape of digestive diagnostics.
MRI uses a strong magnetic field and radio waves, not X-rays, to create highly detailed images of soft tissues like the bowel wall, liver, pancreas, and bile ducts. For people who want answers without invasive scopes or radiation, it can be a powerful (and often underused) tool.
What MRI Can See in Your Digestive System
Modern abdominal and GI MRI can detect a wide range of conditions that affect how your gut responds to food and why certain meals set off flares. It does not replace every test, but it often provides a high-resolution “map” of structures and inflammation that other imaging can miss.
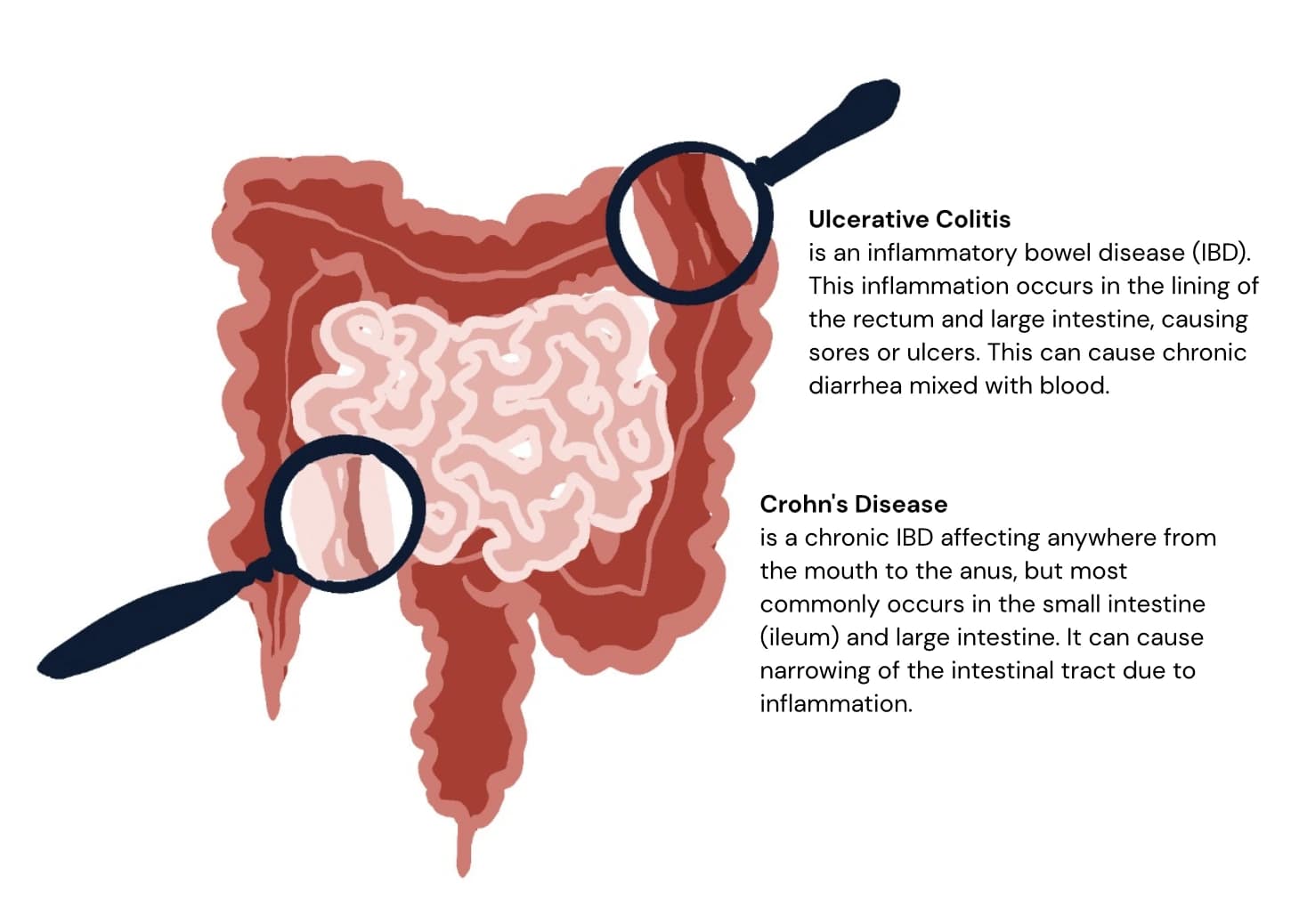
1. Inflammatory Bowel Disease (Crohn's and Ulcerative Colitis)
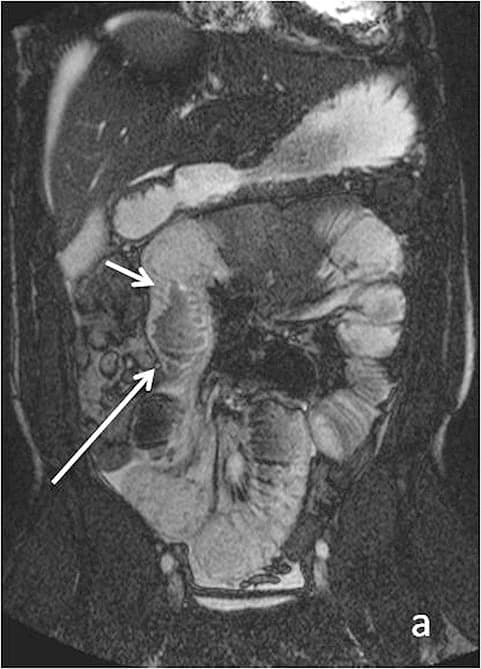
Magnetic resonance enterography (MRE) is now a key test for suspected or known Crohn's disease and, in some contexts, ulcerative colitis.
What MRI shows:
- Active inflammation in the bowel wall (thickening, increased blood flow, edema).
- Strictures (narrowed segments) that can slow or block food passage.
- Fistulas (abnormal tunnels) and abscesses around the intestines.
For someone whose “IBS” is actually undiagnosed Crohn's, these scans can change everything, from diet advice to the need for medication that targets inflammation rather than just masking symptoms.
2. Cancers and Tumors
MRI is widely used to evaluate:
- Liver tumors (benign and malignant) and cirrhosis, often with specialized contrast sequences that distinguish different tissue types.
- Pancreatic tumors and small peritoneal implants that may not be visible on CT or even at laparoscopy.
- Bowel and peri-intestinal tumors, including masses that narrow or obstruct the intestine.
For many liver and biliary tumors, MRI is considered one of the best imaging standards because it can better characterize lesions than CT in many scenarios. Early detection here can dramatically influence treatment options and survival.
3. Inflammations: Appendicitis, Diverticulitis, and Abscesses
MRI can identify acute inflammatory conditions that might otherwise require CT:
- Appendicitis. MRI can show an enlarged, inflamed appendix and surrounding fat stranding, and is especially useful in younger or pregnant patients where avoiding radiation matters.
- Diverticulitis. MRI reveals inflamed diverticula, thickened colon wall, and surrounding fat changes, and can help distinguish diverticulitis from colon cancer.
- Abscesses. Collections of pus in the abdomen or pelvis appear as fluid pockets with characteristic signals and rim enhancement.
These conditions are key to catch early; left untreated, they can cause severe pain, systemic infection, and emergency surgery.
4. Bowel Obstruction and Motility Problems
MRI can help identify:
- Mechanical obstruction. Dilated loops of bowel with a clear transition point where something (a stricture, mass, or adhesion) is blocking flow.
- Functional slow-down. While MRI is less commonly used than other tests for motility, dynamic sequences can show slowed transit or dysmotility in selected centers.
For someone whose life revolves around constipation, bloating, or sudden vomiting, ruling in or out a structural obstruction is a major step toward the right treatment.
5. Pancreatic and Biliary Tract Problems
Specialized sequences like MRCP (magnetic resonance cholangiopancreatography) provide a duct-level view of the pancreas, gallbladder, and bile ducts.
MRI/MRCP can identify:
- Pancreatitis and pancreatic cysts (which may or may not be cancerous).
- Bile duct stones and strictures, including blockages that may cause jaundice, pain, or pale stools.
- Anatomical variants of the ducts that predispose to recurrent pancreatitis or pain.
These conditions often present with upper abdominal pain, nausea, and food-triggered flares, and MRI can pinpoint the structural cause.
6. Liver Disease
Beyond tumors, liver MRI can:
- Detect and characterize cirrhosis (scarring of the liver) and its complications.
- Assess fatty liver disease and iron overload using quantitative techniques.
Because metabolic risk factors (obesity, diabetes, high cholesterol) are common in adults, this type of imaging can uncover liver contributions to fatigue, abdominal discomfort, and systemic symptoms before they progress.
What MRI Cannot (and Should Not) Do
Despite its power, MRI cannot answer every question, especially those about how your body responds to specific foods. Understanding its limits helps you combine it wisely with other tests.
- Microscopic inflammation without structural change. Conditions like microscopic colitis or early celiac disease may have a normal appearance on MRI because they primarily affect the mucosal lining at a microscopic level. Endoscopy with biopsies is usually required.
- Mild functional disorders. By definition, these often lack visible structural abnormalities. MRI can help exclude serious organic disease (Crohn's, tumors, strictures), but it will frequently look “normal” in IBS.
- Very small polyps or early mucosal cancers. Colonoscopy and upper endoscopy are still the gold standards for detecting small polyps, flat lesions, and early mucosal cancers because they allow direct visualization and biopsy.
Depending on your symptoms, a clinician might pair or prioritize other tools such as endoscopies or colonoscopies that directly inspect the linings, or breath tests and lab work to assess food sensitivities and tolerances.
The right combination depends on your specific symptoms, risk factors, and what the clinician is trying to rule in or out. MRI often shines as a second-line, problem-solving, or follow-up tool when you want deeper structural information without added radiation.
Turning Curiosity Into Action
If you're living with persistent digestive issues, it's reasonable to want some definitive answers. Here is what a practical path often looks like (remember to discuss details with your clinician):
- Clarify your symptom pattern and red flags. Duration, triggers, alarm signs (bleeding, weight loss, fevers, nighttime pain) help determine urgency and which tests matter most.
- Start with targeted basic tests. Blood work, stool tests, and in many cases endoscopy/colonoscopy can rule out common mucosal diseases.
- Use MRI when structural questions remain. For example:
- “Is this long-standing ‘IBS’ actually Crohn's?” → MRE.
- “Do I have a stricture, fistula, or abscess explaining these severe flares?” → GI MRI/MRE.
- “Could this upper abdominal pain be from the pancreas or bile ducts?” → MRI/MRCP.
- “What exactly is this liver lesion, and do I have cirrhosis or fatty liver?” → Liver MRI with contrast.
- Adjust diet and lifestyle with real data. Once serious structural disease is ruled in or out, you can work with a gastroenterologist and dietitian to tailor your diet, physical activity, and stress management, without the nagging fear that you might be missing something major.
For many people, the biggest gift of modern MRI is the ability to say with confidence, “Here's what's going on in your gut, and here's what you don't have to worry about.” That clarity can transform how you eat, travel, work, and plan your life, turning a vague unease into informed choices and genuine peace of mind.
References
[1] Burisch, J., & Munkholm, P. (2015). The epidemiology of inflammatory bowel disease. Scandinavian Journal of Gastroenterology, 50(8), 942–951. link
[2] Drossman, D. A., & Hasler, W. L. (2016). Rome IV—Functional GI Disorders: Disorders of Gut-Brain Interaction. Gastroenterology, 150(6), 1257–1261. link
[3] Everhart, J. E., & Ruhl, C. E. (2009). Burden of digestive diseases in the United States part I. Gastroenterology, 136(2), 376–386. link
[4] Ford, A. C., Lacy, B. E., & Talley, N. J. (2017). Irritable Bowel Syndrome. The New England Journal of Medicine, 376(26), 2566–2578. link
[5] Chuah, K. H., & Mahadeva, S. (2018). Cultural Factors Influencing Functional Gastrointestinal Disorders in the East. Journal of Neurogastroenterology and Motility, 24(4), 536–543. link
[6] Maccioni, F., et al. (2023). Magnetic Resonance Imaging of the Gastrointestinal Tract. Diagnostics, 13(14), 2410. link
[7] Sperber, A. D., et al. (2021). Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders. Gastroenterology, 160(1), 99–114.e3. link
[8] Amitai, M. M., et al. (2013). Magnetic resonance enterography in Crohn's disease. Journal of Crohn's & Colitis, 7(8), 603–615. link
[9] Quigley, E. M. M. (2017). Microbiota-Brain-Gut Axis and Neurodegenerative Diseases. Current Neurology and Neuroscience Reports, 17(12), 94. link
[10] Taylor, S. A., et al. (2019). Magnetic resonance enterography compared with ultrasonography in Crohn's disease patients: the METRIC diagnostic accuracy study. Health Technology Assessment, 23(42), 1–162. link
[11] Chezmar, J. L. (1991). Magnetic resonance imaging of the liver. Radiologic Clinics of North America, 29(6), 1251–1258.
[12] Lee, D. I., et al. (2022). Comparison of Diagnostic Performance of Ultrasonography and MRE in Crohn's Disease. Diagnostics, 12(8), 2008. link
[13] Almario, C. V., et al. (2018). Burden of Gastrointestinal Symptoms in the United States. The American Journal of Gastroenterology, 113(11), 1701–1710. link