
Kidney stones are common, extremely painful, and largely linked to how concentrated your urine is.
These affect approximately one in eleven people in the United States, with prevalence doubling over the past several decades. They form when minerals and salts in your urine crystallize and clump together, which happens more easily if you're dehydrated, eat a lot of salt and animal protein, or have certain medical or genetic risk factors.
What Kidney Stones Are and How They Show Up
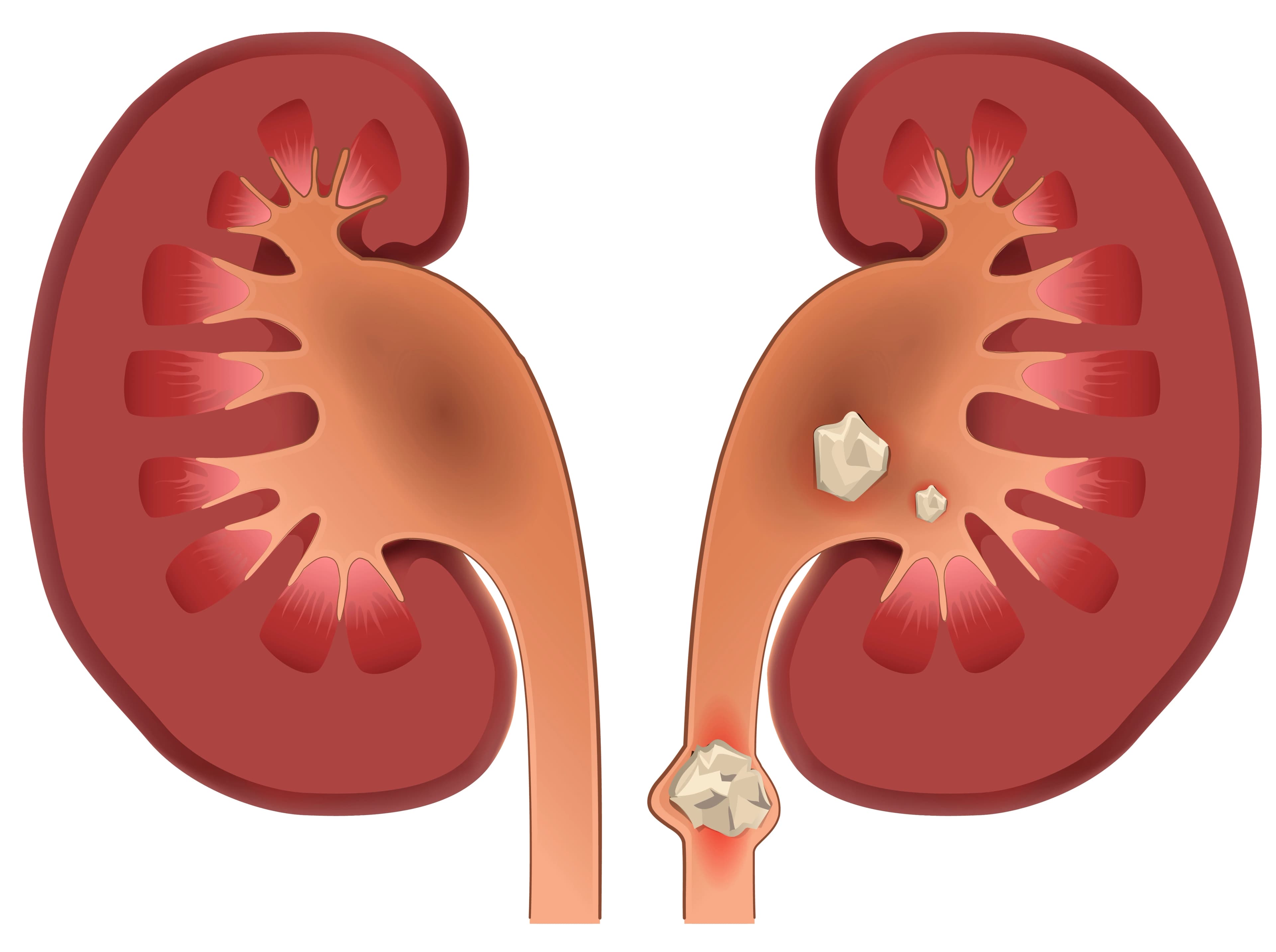
Kidney stones are hard “pebbles” that can be as small as a grain of sand or big enough to block the flow of urine.
Pain occurs when a stone gets stuck in one of the ureters, blocking the flow of urine and causing the kidney to swell and the ureter to spasm.
They usually stay silent in the kidney until they start moving; then they can cause sudden, severe pain that shoots from your side or back down toward your groin, often with nausea and blood in the urine.
The kidney's role as a filtration system makes it particularly vulnerable to stone formation. As blood passes through the kidneys, waste products and excess minerals concentrate in the urine.
When fluid intake is insufficient or certain substances become overly concentrated, crystallization begins. These crystals can remain microscopic and pass unnoticed, or they can grow and adhere to kidney surfaces, developing into problematic stones.
How Dehydration and Diet Cause Kidney Stones

Most stones are driven by a mix of dehydration, diet, and individual susceptibility rather than one single cause. Not drinking enough fluid makes the urine concentrated so minerals like calcium, oxalate, and uric acid are more likely to crystallize. In the modern day and age, our high-salt, high meat diets push more calcium and uric acid into the urine, lowering helpful “stone blockers” like citrate.
High-risk foods when consumed in excess:
- Heavily salted and processed foods
- Large portions of meat (especially red meat and organ meats)
- High-oxalate items: spinach, rhubarb, nuts, chocolate, strong tea
- High-dose vitamin C supplements (converts to oxalate)
Conditions such as obesity, gout, some bowel diseases, and certain inherited disorders push risk higher still.
A Simple Picture of Testing and Treatment
Because other illnesses, like appendicitis, gallbladder attacks, or muscle strains, can mimic stone pain, imaging is usually needed to be sure. A non-contrast CT scan is the most accurate test, but ultrasound is often used first, especially in younger people and pregnancy, to avoid radiation.
Small stones often pass on their own with time, pain control, and plenty of fluids; medications that relax the ureter can help some people pass stones faster.
Larger stones, stones that don't move, or stones causing infection or kidney damage usually need a procedure, such as using a scope and laser through the bladder, breaking the stone with focused sound waves, or, for very large stones, removing them through a small incision in the back.
Everyday Ways to Prevent Stones
The good news is that simple, consistent habits can significantly cut the odds of getting a stone, or of having another one if you've already had one.
- Drink more fluid. Aim for enough that you produce at least about 2.5 liters of urine per day; in practice, that often means about 2–3 liters of fluid (ideally water) spread through the day, with extra when it's hot or you're sweating.
- Consume calcium in your diet, don't cut it. Getting normal amounts of calcium from foods like dairy actually lowers the chance of calcium stones by binding oxalate in the gut, while very low-calcium diets raise stone risk.
- Ease up on salt. Limiting sodium (especially from processed foods and restaurant meals) helps keep calcium levels in the urine down and makes stones less likely.
- Moderate animal protein intake. Large amounts of meat, poultry, and seafood can acidify urine and increase uric acid and calcium stone risk; shifting toward more plant-based protein helps.
- Be smart about high-oxalate foods. If you form calcium oxalate stones, go “light but not zero” on very high-oxalate items (like large daily portions of spinach or rhubarb) and eat them together with calcium-containing foods when you do have them.
- Maintain a healthy weight and manage other conditions. Separately addressing obesity, blood pressure, and gout lowers stone risk and improves heart health at the same time.
People with repeated stones or unusual stone types often need tailored help, including stone analysis and a 24-hour urine test. In those cases, targeted medicines can lower calcium in urine, raise citrate, lower uric acid and reduce recurrences.
Proactively Address the “Red Flags” in Your Health
A kidney stone is rarely a one-off event. Without changes, many people will have another stone in the next few years, and the same underlying patterns, like high blood pressure, insulin resistance, and excess weight, also increase the risk of heart disease and other problems.
Treating a stone is not just about getting through one painful episode. It's a chance to rethink hydration, diet, and overall health.
Curiosity Fact-Sheets
Fact Sheet 1: Diagnostic Challenge — What Kidney Stones Can Mimic
Kidney stone diagnosis can be surprisingly complex because several conditions produce similar symptoms.
| Condition | Kidney Stone Symptoms | Key Clues That Suggest A Different Condition |
|---|---|---|
| Urinary tract infection (UTI) | Flank or lower abdominal pain, burning with urination, frequent urges to urinate, sometimes blood in the urine. | Often has fever, cloudy or foul-smelling urine, and more generalized “sick” feeling or fatigue. |
| Appendicitis | Right-sided abdominal pain that can be severe and may radiate, sometimes with nausea. | Pain usually starts near the belly button, moves to the right lower abdomen, worsens with movement or coughing, and is tender to press in one spot. |
| Gallstones | Severe pain in the upper right abdomen or mid-upper abdomen that can radiate to the back, nausea or vomiting. | Pain often triggered or worsened after fatty meals and may be accompanied by jaundice (yellowing of skin or eyes). |
| Diverticulitis | Lower abdominal pain, often left-sided, sometimes with fever and bowel changes. | Pain tends to stay in the lower abdomen rather than radiating from the flank toward the groin, and may come with constipation or diarrhea. |
| Ovarian cyst (rupture or torsion) | Sudden, sharp pelvic or lower abdominal pain on one side that can be severe. | Occurs only in people with ovaries, often linked to menstrual or reproductive history; may have tenderness over the ovary and gynecologic findings on exam or ultrasound. |
| Musculoskeletal pain | Back or flank pain that can feel sharp or intense. | Pain usually changes with movement, posture, or pressing on muscles; often improves or worsens with certain positions rather than staying constant like classic renal colic. |
Fact Sheet 2: Microscopic Architecture — 3 Ways Kidney Stones Form
The pathophysiology of kidney stone formation involves three primary pathways, each reflecting different underlying mechanisms.
| Formation Pathway | What Happens in the Kidney | When It's More Likely |
|---|---|---|
| Randall's plaques [most common] | Tiny calcium phosphate deposits build up under the inner lining of the kidney; over time they break through the surface and act like “seeds” where calcium oxalate crystals stick and grow into stones. | Very common in typical calcium oxalate stone formers; risk rises when urine is concentrated with calcium and oxalate and low in natural inhibitors like citrate and magnesium. |
| Mineral plugs in ducts of Bellini | Crystals form inside the kidney's tiny tubules and create “plugs” that protrude into the collecting ducts; stones then grow on these plugs. | Seen more often in conditions such as high oxalate levels (hyperoxaluria) or certain acid–base problems (e.g., distal renal tubular acidosis). |
| Free-floating crystallization | Crystals form directly in the urine within the collecting system and stick together into stones without needing a plaque or plug. | Typical of some rarer stone types like cystine stones and can occur when urine is heavily loaded with stone-forming substances and low in inhibitors. |
References
[1] American Academy of Family Physicians. (2019). Kidney stones: Diagnosis, treatment, and prevention. American Family Physician, 99(8), 490–496.
[2] Borghi, L., et al. (1996). Urinary volume, water and recurrences in idiopathic calcium nephrolithiasis: a 5-year randomized prospective study. The Journal of Urology, 155(3), 839–843.
[3] Curhan, G. C., et al. (1993). A prospective study of dietary calcium and other nutrients and the risk of symptomatic kidney stones. The New England Journal of Medicine, 328(12), 833–838. link
[4] Edvardsson, V. O., et al. (2013). Hereditary causes of kidney stones and chronic kidney disease. Pediatric Nephrology, 28(10), 1923–1942. link
[5] Hollingsworth, J. M., et al. (2006). Medical therapy to facilitate urinary stone passage: a meta-analysis. Lancet, 368(9542), 1171–1179. link
[6] Moe, O. W. (2006). Kidney stones: pathophysiology and medical management. Lancet, 367(9507), 333–344. link
[7] InformedHealth.org, Institute for Quality and Efficiency in Health Care (IQWiG). Kidney stones: Preventing kidney stones. link
[8] Scales, C. D. Jr., et al. (2012). Prevalence of kidney stones in the United States. European Urology, 62(1), 160–165. link
[9] Smith-Bindman, R., et al. (2014). Ultrasonography versus computed tomography for suspected nephrolithiasis. The New England Journal of Medicine, 371(12), 1100–1110. link


