You're 27 and exhausted. But so is everyone in your friend group, so you brush it off.
Maybe your foot has been buzzing when you cross your legs. Maybe your vision went briefly blurry one morning and you blamed it on a long night of staring at a screen. Maybe a hand went numb in yoga class and you shook it off as a weird sleep position.
For most women, those moments mean nothing at all. For some, they are the first soft signals that something autoimmune has just switched on.
Women between 20 & 40 are the most likely group to receive a new multiple sclerosis diagnosis, and they are the fastest-growing demographic for almost every autoimmune disease tracked in the United States.
Women are roughly three to four times more likely than men to develop MS, and overall, women carry around 80% of the autoimmune disease burden in the country.
This is not to say every neurological hiccup is MS. It is just that the moment in life where these conditions tend to first show themselves, for many women, is exactly the moment most are too busy to take them seriously.
What Is Actually Happening When Autoimmunity Begins
Autoimmunity is, at its core, a case of mistaken identity. The immune system, which is built to identify and attack invaders, starts targeting healthy tissue instead.
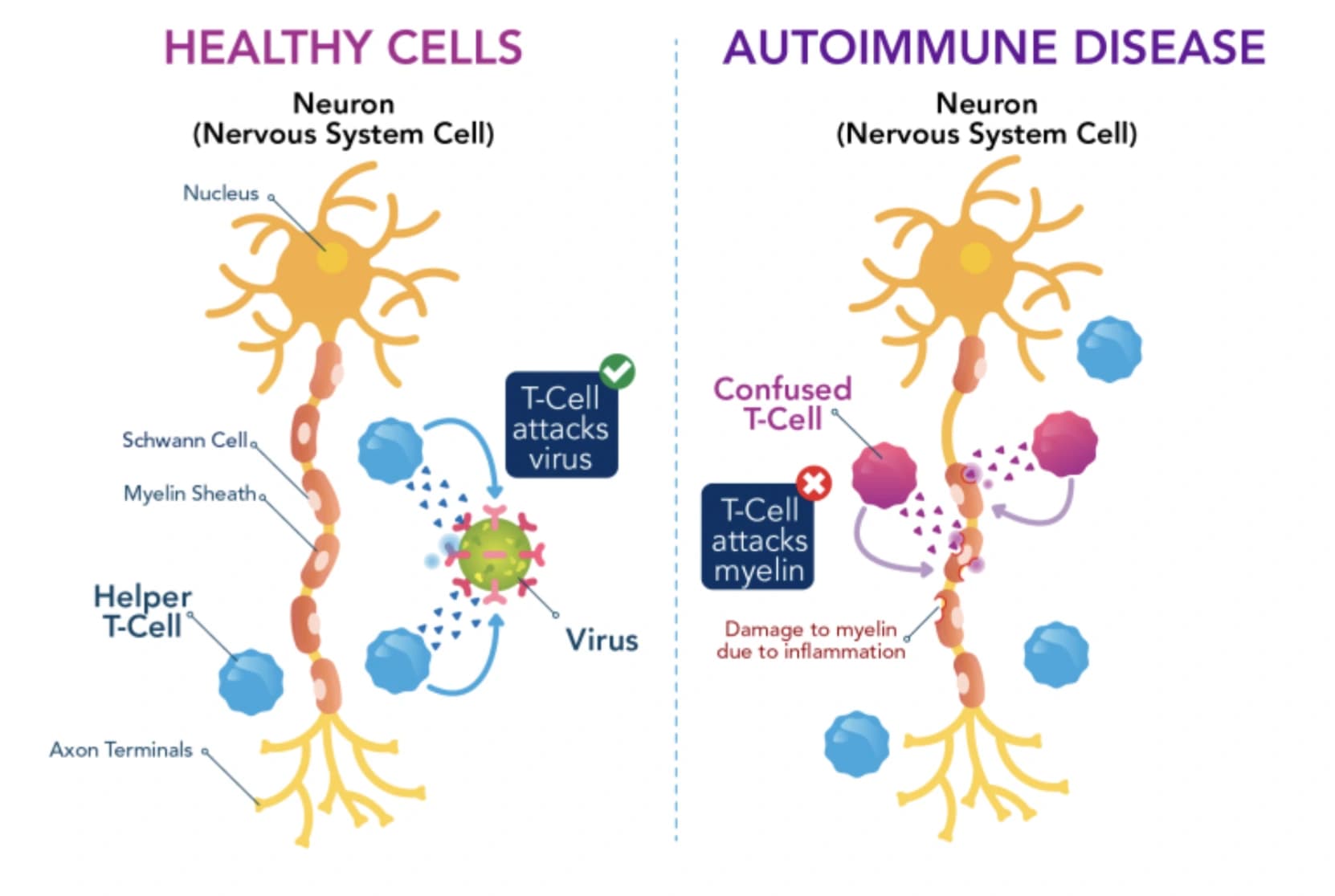
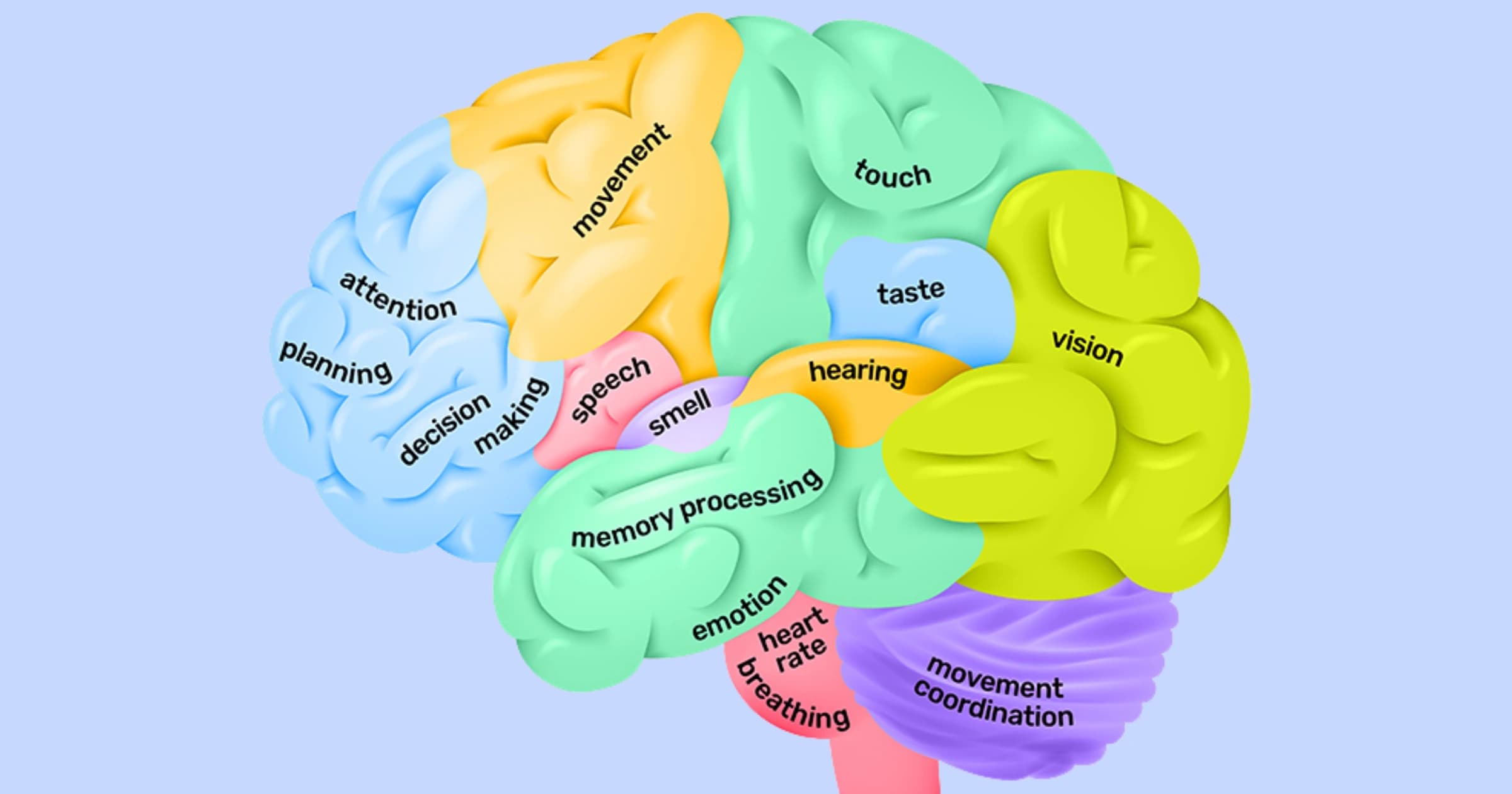
In MS, the target is myelin, the fatty insulation that wraps your nerve fibers like rubber around an electrical cord. When myelin is attacked, signals in the brain and spinal cord slow or short-circuit, and the result is the strange, often intermittent collection of symptoms MS is known for: numbness, fatigue, vision changes, weakness, balance issues, even cognitive fog that's hard to put your finger on.
The same phenomenon goes by many names:
- In lupus, the target is connective tissue.
- In Hashimoto's, the thyroid.
- In rheumatoid arthritis, the lining of the joints.
- In celiac, the small intestine.
The mechanism is the same: the body misidentifies a piece of itself as foreign, and the inflammation that follows, when left unchecked, becomes the disease.
Why Women, and Why Now
Researchers have long suspected hormones, the X chromosome, and immune sensitivity in women's bodies are all playing a role, and recent work has pointed sharper fingers.
The X chromosome carries a high concentration of immune-related genes, and women have two of them. Genetic redundancy is usually protective, but here it tilts the immune system toward overreaction.
Estrogen and progesterone modulate immune function in complex ways. Pregnancy, postpartum, & perimenopause are common windows where autoimmune activity flares or first appears, which is why so many women look back and trace the start of their symptoms to a pregnancy or a particularly stressful year.
And in 2022, a landmark study from Harvard published in Science offered the strongest evidence yet that Epstein-Barr virus is a likely trigger for MS. The study tracked over 10 million U.S. military members and found that EBV infection raised the risk of developing MS 32-fold. Since the vast majority of adults have had EBV by their mid-twenties, often as the kissing virus or mono in college, this finding helps explain why MS so often begins in young adulthood.
What MS Often Looks Like in the Beginning
MS rarely announces itself loudly. The earliest signs tend to be vague enough that most women dismiss them, and reasonable enough that many general practitioners do too.
A few of the most common early symptoms to know:
- Optic neuritis, a sudden blurring or partial loss of vision in one eye, often with eye pain when looking side to side. This is one of the most frequent first symptoms and is often mistaken for migraine or eye strain.
- Lhermitte's sign, an electric-shock sensation that runs down the spine when bending the neck forward.
- Persistent fatigue that doesn't match your level of exertion, especially the kind that worsens with heat or after exercise.
- Numbness or tingling in a limb or part of the face that lasts days to weeks rather than seconds.
- Trouble with fine motor tasks, balance, or coordination that comes and goes.
The defining feature of early MS is that symptoms tend to come, go, & migrate. One arm tingles for three weeks, resolves, and three months later something feels off in a leg.
This isn't a checklist for self-diagnosis, but something worth keeping in mind when something keeps quietly recurring.
What Medicine in 2026 Can Actually Do
The MS landscape today looks dramatically different than it did even ten years ago, and the shift has been a good one.
The old model was “wait and see,” starting patients on mild medications and escalating only as the disease progressed. The current evidence strongly favors early, aggressive treatment.
Data from large international registries like MSBase show that patients started on high-efficacy therapies within two years of their first symptoms have meaningfully better long-term outcomes than those treated reactively.
New therapies in late-stage trials include BTK inhibitors which target a different arm of the immune system entirely and may slow the progressive forms of MS.
The diagnostic side has moved just as fast. The updated McDonald Criteria now allow for an earlier confident MS diagnosis using MRI evidence alone in some cases, and 7T MRI scanners are increasingly able to spot the small lesions and “central vein signs” that earlier generations of machines simply missed.
The window for changing the long-term trajectory of MS is widest in the first few years after symptoms begin. That window only matters, however, if the disease is actually caught.
Get Diagnosed With MRI
MS is, fundamentally, an imaging diagnosis as much as a clinical one.
Blood tests can support the picture. A spinal tap can add weight. But MRI is the only tool that lets clinicians actually see the demyelinating lesions in the brain and spinal cord that define the disease.
A modern brain and spine MRI can:
- Reveal active, contrast-enhancing lesions that indicate inflammation happening right now.
- Show older lesions that point to past silent attacks, which helps establish the “dissemination in time and space” that a confident MS diagnosis requires.
- Detect changes characteristic of conditions that mimic MS, including small vessel disease, vasculitis, neuromyelitis optica, and other autoimmune neurological conditions that all require very different treatment.
For autoimmune neurological symptoms more broadly, MRI is often what separates a real lead from a guess. A neurologist's strongest tool, especially before symptoms have organized into a clear pattern, is a high-quality image to compare against.
This is also where a full-body MRI can be quietly useful. For women navigating vague autoimmune symptoms, having a clear baseline image to compare against years later can shave significant time off a diagnostic process that, on average, still takes over a year from symptom onset to MS diagnosis.
A Few Honest Caveats
Most numbness, fatigue, and visual blurring in young women is not MS. Anxiety, iron deficiency, low vitamin D, thyroid imbalance & chronic sleep loss all produce strikingly similar patterns. There is no need to panic at every twinge, just make a mental note to take repeating, unexplained symptoms seriously rather than rationalizing them away.
MRI findings can also be genuinely ambiguous. Small white matter spots are common with age, migraines, and elevated blood pressure, and they do not always indicate MS. A skilled neuroradiologist's read matters more than the image alone, which is why where you scan matters as much as whether you scan.
And not every autoimmune condition is preventable or fully treatable. What is increasingly possible is early detection, smarter treatment selection, and meaningfully better long-term outcomes. That's a different promise than a cure, but it's an honest one, and for most women it is the one that actually changes things.
Walk Away With This
Though statistically the strongest & healthiest, the decade between 25 and 35 is quietly one of the most important medical decades of a woman's life. Many autoimmune diseases begin in that stretch and many of them, especially MS, have early-treatment windows that close faster than the diagnostic system tends to move.
If something has been off for more than a few weeks, particularly anything neurological, it's worth investigating before it becomes a pattern you can chart in hindsight.
Most of the time, you'll find that nothing serious is going on, and you'll get to put the worry down. Some of the time, you'll catch something early enough that the difference between treating now and treating later is the rest of your life.
It is far easier to disprove a worry than to undo a missed opportunity.
Citations
[1] Bjornevik, K., Cortese, M., Healy, B. C., et al. (2022). Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science, 375(6578), 296–301. link
[2] Thompson, A. J., Banwell, B. L., Barkhof, F., et al. (2018). Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. The Lancet Neurology, 17(2), 162–173. link
[3] He, A., Merkel, B., Brown, J. W. L., et al. (2020). Timing of high-efficacy therapy for multiple sclerosis: a retrospective observational cohort study. The Lancet Neurology, 19(4), 307–316. link
[4] Fairweather, D., & Rose, N. R. (2004). Women and autoimmune diseases. Emerging Infectious Diseases, 10(11), 2005–2011. link